
While the year is almost at end, we still have a number of studies published that we have not shared. Amongst those, this cost-effectiveness analysis of the 11+Kids Football Injury Prevention Program. Not your straightforward cost-effectiveness analysis … this one looks broader and evaluates the potential reduction in injury related healthcare costs on a national level (Swiss in this case) when implementing the ’11+ Kids’ injury prevention programme.
This cost effectiveness analysis was based on data collected in a cluster randomised controlled
trial over one season, with 1,002 Swiss football players in under-9 to under-13 age teams. The intervention group replaced their usual warmup with ’11+ Kids’, while the control group warmed up as usual. Injuries, healthcare resource use and football exposure (in hours) were collected prospectively. We calculated the mean injury related costs in Swiss Francs (CHF) per 1,000 hours of football. We calculated the cost effectiveness (the direct net healthcare costs divided by the net health effects of the ’11+ Kids’ intervention) based on the actual data in our study (trial based) and for a countrywide implementation scenario (model based).
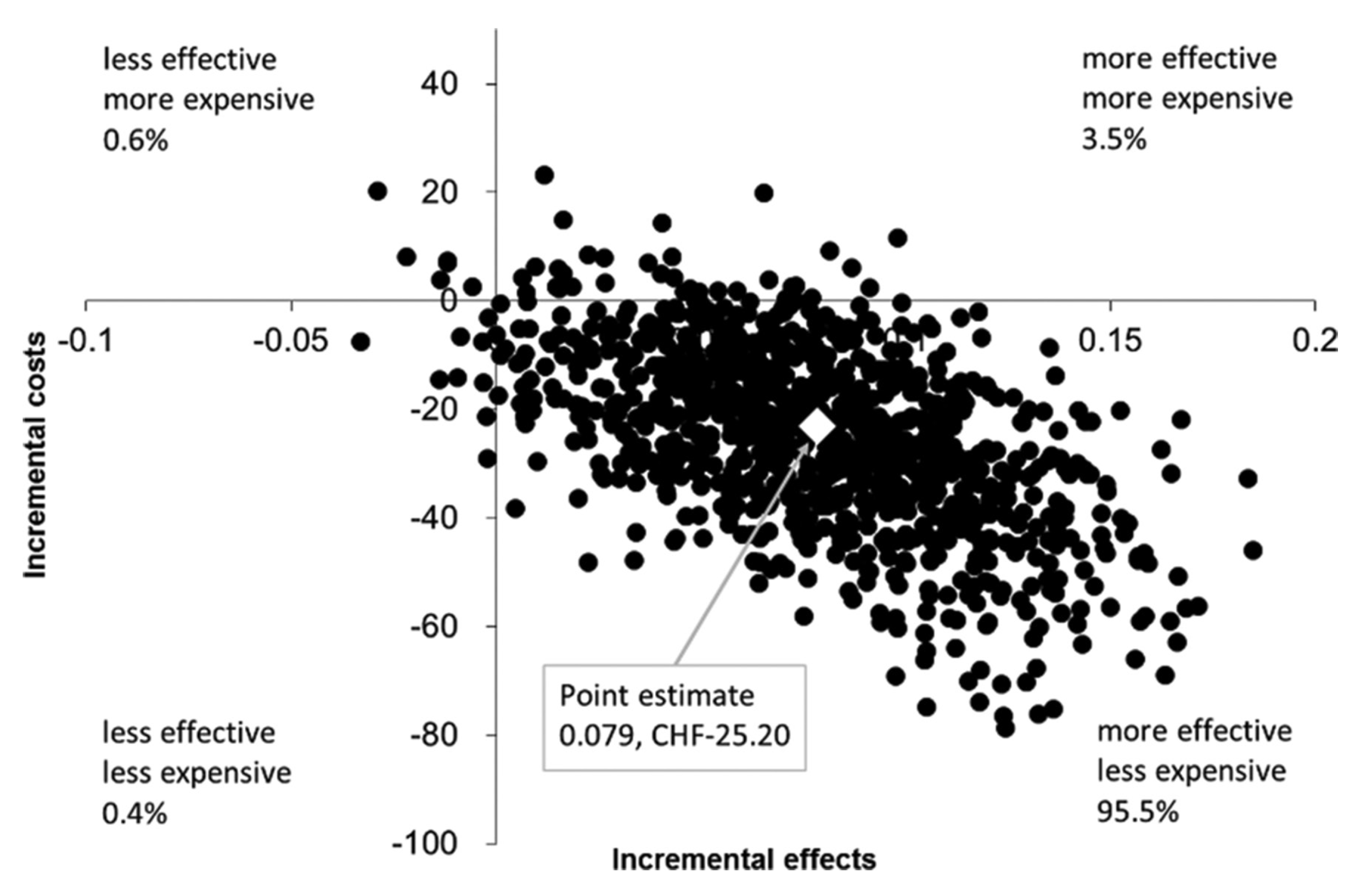
Cost effectiveness plane presenting model based data for a countrywide implementation of the ‘11+ Kids’. Cost effect pairs were estimated using bootstrapping (1,000 samples) for the difference in the costs and injury risk in the ‘11+ Kids’ intervention group versus the control group. The figure shows simulated data for a countrywide implementation scenario in Switzerland over one football season. Values in the southeast (dominant) quadrant indicate that the intervention group showed lower costs and lower injury incidence density. Data in the northwest quadrant (dominated) indicate that the intervention group showed higher costs and a higher injury incidence density.
Costs per 1,000 hours of exposure were CHF 228.34 (95% CI 137.45, 335.77) in the 11+Kids group and CHF 469.00 (95% CI 273.30, 691.11) in the control group. The cost difference per 1,000 hours of exposure was CHF−240.66 (95%CI −406.89, −74.32). A countrywide implementation would reduce healthcare costs in Switzerland by an estimated CHF 1.48 million per year.
Some take home points
The ‘11+ Kids’ programme reduced the injury related healthcare costs by 51% in players aged 7–12 years.
The cost effectiveness analysis showed a 94.6% likelihood (trial based data) and a 95.5% likelihood (model based implementation scenario) for ‘11+ Kids’ being dominant (ie, more effective and less costly) over usual warmup.
A countrywide application of ‘11+ Kids’ in Switzerland could prevent approximately 2500 medically treated injuries and save CHF 1.48 million in direct healthcare costs per year.
The clear reduction in injury related costs provides strong evidence for a widespread implementation of the ‘11+ Kids’.
The full article can be accessed here (open access)
Rössler R, Verhagen E, Rommers N, Dvorak J, Junge A, Lichtenstein E, et al. Comparison of the '11+ Kids‘ injury prevention programme and a regular warmup in children’s football (soccer): a cost effectiveness analysis. Br J Sports Med. 2018 Online First